“Not all patients with upper abdominal pain need an endoscopy,” emphasizes Professor di Mario, highlighting the importance of non-invasive diagnostics.
Non-invasive methods can achieve significant screening benefits and cost-effectiveness, stressed Professor Francesco di Mario from the University of Parma during his lecture on atrophic gastritis and its diagnostics on November 29, 2024, at the Internal Medicine Doctors’ Days in Helsinki.
The lecture described the epidemiology, pathophysiology, and findings in atrophic gastritis, and options for diagnostics, treatment and follow-up. Professor Francesco di Mario was present at the invitation of Biohit.
Read this summary of the professor’s key insights related to atrophic gastritis and its diagnostics.
Key points include:
- Early diagnosis can save lives in cases of stomach cancer.
- GastroPanel® offers a reliable non-invasive diagnostic tool.
- H. pylori eradication therapy is an effective long-term strategy.
- L-cysteine offers a new potential treatment option.
Atrophic gastritis develops gradually
In atrophic gastritis, the original, normal glands of the stomach lining are damaged and partially replaced by another type of tissue, known as metaplasia.
The Correa’s Cascade model describes the progression of the disease:
- H. pylori infection often acts as a trigger.
- Achlorhydria develops.
- The disease progresses to a point of no return.
- Untreated achlorhydria can lead to stomach cancer.
Professor di Mario considers the European situation in stomach cancer diagnosis particularly significant:
In Japan, 80% of stomach cancers are found at an early stage, while in Europe, 60-80% are diagnosed at an advanced stage. This difference is also reflected in the prognosis: with early-stage diagnosis, the 5-year survival rate is 90%, while with late-stage diagnosis, it is only 10%.
GastroPanel offers a reliable diagnostic tool
Di Mario emphasized the importance of the blood sample-based GastroPanel test in selecting patients for gastroscopy. “Not all patients with upper abdominal pain need an endoscopy. With GastroPanel, we can screen those who truly need an endoscopy from a blood sample,” he notes.
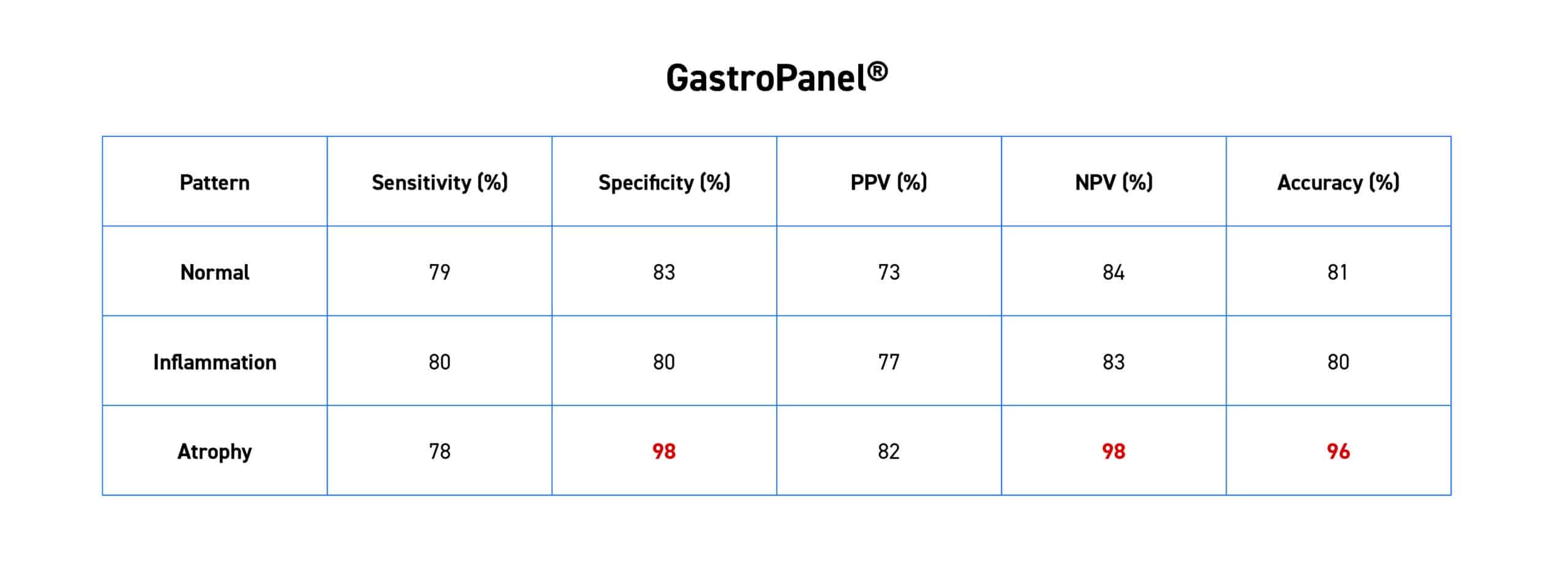
Research data shows the diagnostic accuracy of GastroPanel:
- Specificity of 98% and negative predictive value of 98% in identifying atrophy.
- Sensitivity of 79% and specificity of 83% in identifying normal findings.
- Both sensitivity and specificity of 80% in identifying inflammation.
The long-term results of Helicobacter pylori eradication therapy are convincing
In the context of atrophic gastritis, Helicobacter pylori, which can cause achlorhydria, must also be discussed. Professor di Mario presented a comprehensive 25-year follow-up study (n=693) that demonstrated the effectiveness of H. pylori eradication therapy: the risk of disease recurrence is highest in the first five years (3.89%) and decreases thereafter, being lowest in the 20-25 year follow-up (1.30%).
However, H. pylori testing alone is not enough, di Mario underlined. “About half of the world’s population carries the bacterium, but we are only interested in those for whom the bacterium has caused stomach damage.” And this is where the GastroPanel® rapid test provides important answers, as it gives a comprehensive picture of the stomach’s condition.
Di Mario emphasized that several international recommendations already support the use of pepsinogen testing in diagnostics. For example, the Maastricht VI (2022) recommendations confirm their position as the best non-invasive test for diagnosing atrophic gastritis. They also support regular follow-up with both GastroPanel and endoscopies.
Promising results from L-cysteine treatment
As a significant development, the professor presented research results on the use of L-cysteine in treating the symptoms of atrophic gastritis.
The importance of L-cysteine is particularly highlighted by its ability to bind carcinogenic acetaldehyde locally in the stomach: studies show that it binds 60-70% of acetaldehyde in gastric juice after alcohol consumption. This is significant because, in an achlorhydric stomach, acetaldehyde is a key factor for increasing cancer risk.
After L-cysteine administration, patients with atrophic gastritis in the body (corpus) mucosa showed long-lasting improvements in the physiological function of the stomach. This was reflected in a significant increase in PGI levels and a simultaneous decrease in G-17 serum levels during the 48-month follow-up period.
In the 48-month follow-up study (n=46), clear improvements were observed:
- Pepsinogen I levels increased (8.42 → 14.21µg/l)
- Gastrin-17 levels normalized (51.03 → 26.03 pmol/l)
The lecture reinforced the benefits of GastroPanel in the diagnosis and follow-up of atrophic gastritis. Particularly, the role of the test in assessing stomach cancer risk and monitoring treatment response emerged as a key message.
Explore Francesco di Mario’s work on the University of Parma’s website and the research compilation site.
Learn more about the GastroPanel® test ->
(The article and the views, statistics, and recommendations presented in it are based on Professor di Mario’s research and perspectives.)